
Developing Deep Learning Models for Chest X-rays with Adjudicated Image Labels
December 3, 2019
Posted by Dave Steiner, MD, Research Scientist and Shravya Shetty, Technical Lead, Google Health
With millions of diagnostic examinations performed annually, chest X-rays are an important and accessible clinical imaging tool for the detection of many diseases. However, their usefulness can be limited by challenges in interpretation, which requires rapid and thorough evaluation of a two-dimensional image depicting complex, three-dimensional organs and disease processes. Indeed, early-stage lung cancers or pneumothoraces (collapsed lungs) can be missed on chest X-rays, leading to serious adverse outcomes for patients.
Advances in machine learning (ML) present an exciting opportunity to create new tools to help experts interpret medical images. Recent efforts have shown promise in improving lung cancer detection in radiology, prostate cancer grading in pathology, and differential diagnoses in dermatology. For chest X-ray images in particular, large, de-identified public image sets are available to researchers across disciplines, and have facilitated several valuable efforts to develop deep learning models for X-ray interpretation. However, obtaining accurate clinical labels for the very large image sets needed for deep learning can be difficult. Most efforts have either applied rule-based natural language processing (NLP) to radiology reports or relied on image review by individual readers, both of which may introduce inconsistencies or errors that can be especially problematic during model evaluation. Another challenge involves assembling datasets that represent an adequately diverse spectrum of cases (i.e., ensuring inclusion of both “hard” cases and “easy” cases that represent the full spectrum of disease presentation). Finally, some chest X-ray findings are non-specific and depend on clinical information about the patient to fully understand their significance. As such, establishing labels that are clinically meaningful and have consistent definitions can be a challenging component of developing machine learning models that use only the image as input. Without standardized and clinically meaningful datasets as well as rigorous reference standard methods, successful application of ML to interpretation of chest X-rays will be hindered.
To help address these issues, we recently published “Chest Radiograph Interpretation with Deep Learning Models: Assessment with Radiologist-adjudicated Reference Standards and Population-adjusted Evaluation” in the journal Radiology. In this study we developed deep learning models to classify four clinically important findings on chest X-rays — pneumothorax, nodules and masses, fractures, and airspace opacities. These target findings were selected in consultation with radiologists and clinical colleagues, so as to focus on conditions that are both critical for patient care and for which chest X-ray images alone are an important and accessible first-line imaging study. Selection of these findings also allowed model evaluation using only de-identified images without additional clinical data.
Models were evaluated using thousands of held-out images from each dataset for which we collected high-quality labels using a panel-based adjudication process among board-certified radiologists. Four separate radiologists also independently reviewed the held-out images in order to compare radiologist accuracy to that of the deep learning models (using the panel-based image labels as the reference standard). For all four findings and across both datasets, the deep learning models demonstrated radiologist-level performance. We are sharing the adjudicated labels for the publicly available data here to facilitate additional research.
Data Overview
This work leveraged over 600,000 images sourced from two de-identified datasets. The first dataset was developed in collaboration with co-authors at the Apollo Hospitals, and consists of a diverse set of chest X-rays obtained over several years from multiple locations across the Apollo Hospitals network. The second dataset is the publicly available ChestX-ray14 image set released by the National Institutes of Health (NIH). This second dataset has served as an important resource for many machine learning efforts, yet has limitations stemming from issues with the accuracy and clinical interpretation of the currently available labels.
 |
| Chest X-ray depicting an upper left lobe pneumothorax identified by the model and the adjudication panel, but missed by the individual radiologist readers. Left: The original image. Right: The same image with the most important regions for the model prediction highlighted in orange. |
For very large datasets consisting of hundreds of thousands of images, such as those needed to train highly accurate deep learning models, it is impractical to manually assign image labels. As such, we developed a separate, text-based deep learning model to extract image labels using the de-identified radiology reports associated with each X-ray. This NLP model was then applied to provide labels for over 560,000 images from the Apollo Hospitals dataset used for training the computer vision models.
To reduce noise from any errors introduced by the text-based label extraction and also to provide the relevant labels for a substantial number of the ChestX-ray14 images, approximately 37,000 images across the two datasets were visually reviewed by radiologists. These were separate from the NLP-based labels and helped to ensure high quality labels across such a large, diverse set of training images.
Creating and Sharing Improved Reference Standard Labels
To generate high-quality reference standard labels for model evaluation, we utilized a panel-based adjudication process, whereby three radiologists reviewed all final tune and test set images and resolved disagreements through discussion. This often allowed difficult findings that were initially only detected by a single radiologist to be identified and documented appropriately. To reduce the risk of bias based on any individual radiologist’s personality or seniority, the discussions took place anonymously via an online discussion and adjudication system.
Because the lack of available adjudicated labels was a significant initial barrier to our work, we are sharing with the research community all of the adjudicated labels for the publicly available ChestX-ray14 dataset, including 2,412 training/validation set images and 1,962 test set images (4,374 images in total). We hope that these labels will facilitate future machine learning efforts and enable better apples-to-apples comparisons between machine learning models for chest X-ray interpretation.
Future Outlook
This work presents several contributions: (1) releasing adjudicated labels for images from a publicly available dataset; (2) a method to scale accurate labeling of training data using a text-based deep learning model; (3) evaluation using a diverse set of images with expert-adjudicated reference standard labels; and ultimately (4) radiologist-level performance of deep learning models for clinically important findings on chest X-rays.
However, in regards to model performance, achieving expert-level accuracy on average is just a part of the story. Even though overall accuracy for the deep learning models was consistently similar to that of radiologists for any given finding, performance for both varied across datasets. For example, the sensitivity for detecting pneumothorax among radiologists was approximately 79% for the ChestX-ray14 images, but was only 52% for the same radiologists on the other dataset, suggesting a more difficult collection cases in the latter. This highlights the importance of validating deep learning tools on multiple, diverse datasets and eventually across the patient populations and clinical settings in which any model is intended to be used.
The performance differences between datasets also emphasize the need for standardized evaluation image sets with accurate reference standards in order to allow comparison across studies. For example, if two different models for the same finding were evaluated using different datasets, comparing performance would be of minimal value without knowing additional details such as the case mix, model error modes, or radiologist performance on the same cases.
Finally, the model often identified findings that were consistently missed by radiologists, and vice versa. As such, strategies that combine the unique “skills” of both the deep learning systems and human experts are likely to hold the most promise for realizing the potential of AI applications in medical image interpretation.
Acknowledgements
Key contributors to this project at Google include Sid Mittal, Gavin Duggan, Anna Majkowska, Scott McKinney, Andrew Sellergren, David Steiner, Krish Eswaran, Po-Hsuan Cameron Chen, Yun Liu, Shravya Shetty, and Daniel Tse. Significant contributions and input were also made by radiologist collaborators Joshua Reicher, Alexander Ding, and Sreenivasa Raju Kalidindi. The authors would also like to acknowledge many members of the Google Health radiology team including Jonny Wong, Diego Ardila, Zvika Ben-Haim, Rory Sayres, Shahar Jamshy, Shabir Adeel, Mikhail Fomitchev, Akinori Mitani, Quang Duong, William Chen and Sahar Kazemzadeh. Sincere appreciation also goes to the many radiologists who enabled this work through their expert image interpretation efforts throughout the project.
Other posts of interest
-
April 12, 2024
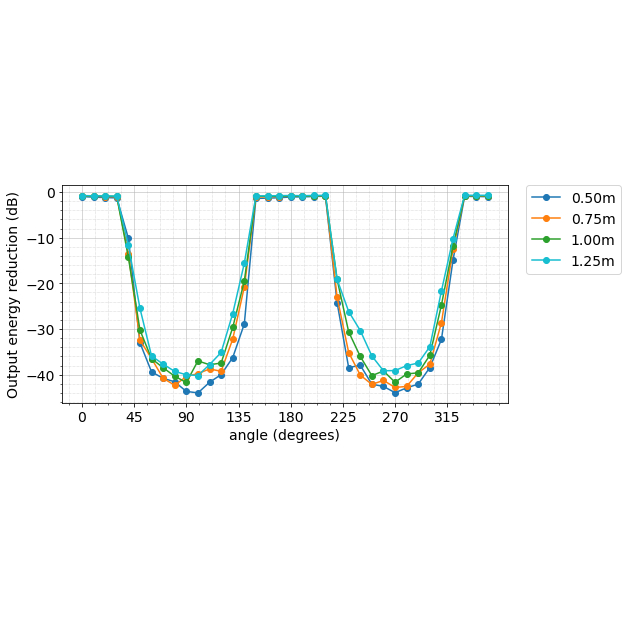
Contrastive neural audio separation- Machine Intelligence ·
- Sound & Accoustics
-
April 11, 2024
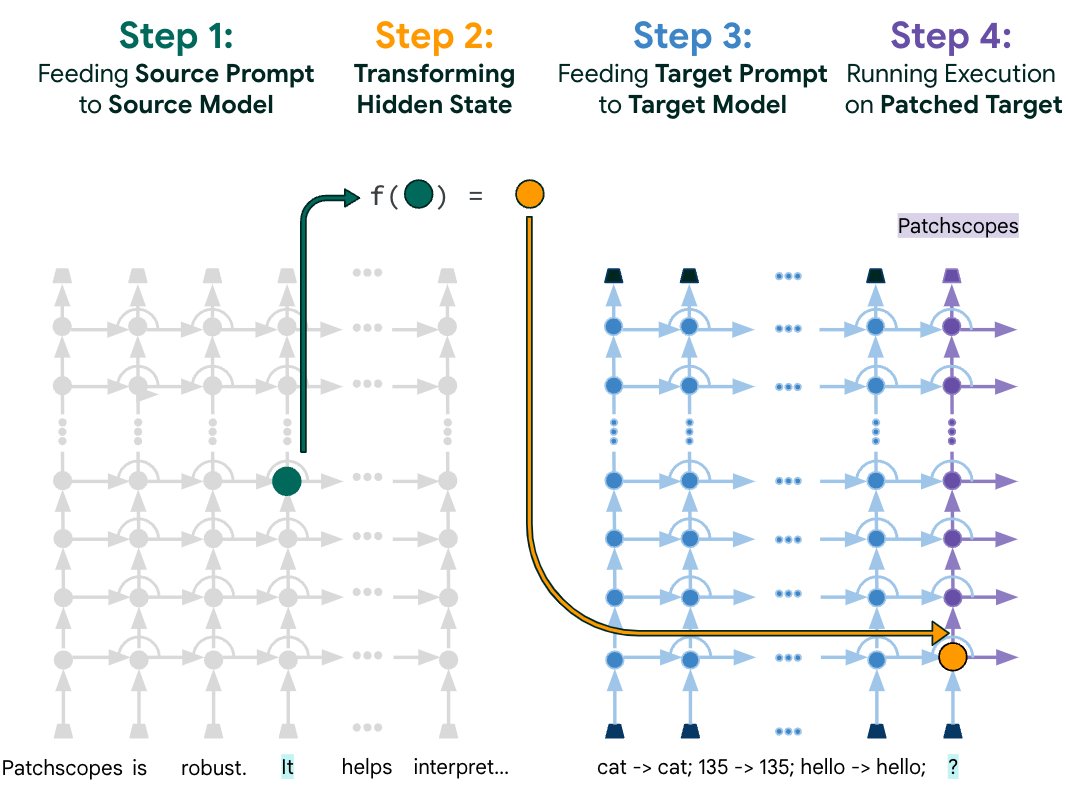
Patchscopes: A unifying framework for inspecting hidden representations of language models- Machine Intelligence ·
- Natural Language Processing ·
- Responsible AI
-
March 28, 2024
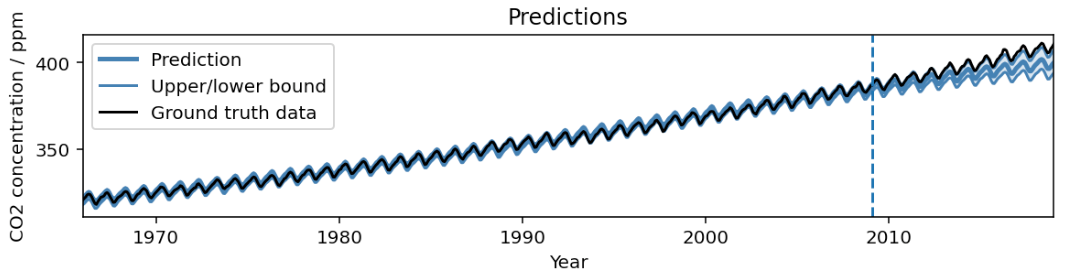
AutoBNN: Probabilistic time series forecasting with compositional bayesian neural networks- Algorithms & Theory ·
- Machine Intelligence ·
- Open Source Models & Datasets